Practice Essentials
Laryngeal manifestations of stroke play a significant role in the morbidity and mortality of stroke, via direct and indirect mechanisms.
The human larynx protects the airway during deglutition, regulates respiration, and facilitates phonation, all of which are vital functions. The unique anatomy (see the images below) and physiology of the larynx, coupled with complex cortical inputs and organized brainstem reflexes, enable the execution of these diverse (and sometimes opposing) tasks. In humans, the high position of the larynx not only facilitates phonation but also compromises its protective and regulatory functions. [1] The effects of stroke on this finely balanced yet inherently precarious system manifest as deficits in swallowing, breathing, and communicating.
Workup in laryngeal manifestations of stroke
The patient’s voice should be assessed while he or she is counting and reading a passage of balanced vowels and consonants. Attention should be paid to the voice’s fluidity (fluid or nonfluid), articulation (clear or indistinct), and the voice quality (normal or raspy, breathy, strained, hypernasal, hyponasal).
Flexible laryngoscopy should be performed while the patient is at rest and during phonation. Before evaluation of the larynx, velopharyngeal function should be visualized with nasopharyngeal endoscopy. Laryngoscopy performed during phonation enables the assessment of laryngeal mobility.
Clinical swallowing examination (CSE), cough reflex testing, fiberoptic endoscopic evaluation of swallowing (FEES), [2] and videofluoroscopic swallow evaluation (VSE) are available tools for assessing aspiration risk.
Evaluation of immobile vocal folds typically includes flexible fiberoptic laryngoscopy and computed tomography (CT) scanning or magnetic resonance imaging (MRI) of the complete course of the recurrent laryngeal nerves; it may also include direct laryngoscopy and palpation of the cricoarytenoid joints, as well as laryngeal electromyography (LEMG).
Videostroboscopy is a critical component of the evaluation in patients with dysphonia. The videostroboscopic examination should include visualization of the larynx during inhalation, cough, sustained vowel (/i/), and sustained vowel with varying degrees of loudness.
Management of laryngeal manifestations of stroke
Dysphagia (medical management)
In patients with dysphagia and intact mental status, dysphagia therapy focuses on techniques to minimize aspiration by increasing anterior laryngeal excursion, the opening of the upper esophageal sphincter, and the pharyngeal clearance. Use of postural maneuvers, different delivery methods (spoon vs cup vs straw), and the alteration of food consistency are other components of dysphagia therapy that may reduce or eliminate aspiration.
Dysphagia (surgical management)
Surgeries that have been described in patients with intractable aspiration include the following [3] :
-
Total laryngectomy
-
Supracricoid partial laryngectomy with cricohyoidoepiglottopexy
-
Tracheoesophageal diversion techniques
-
Various types of supraglottoplasty
-
Tracheostomy with cuffed tracheostomy tube
However, significant impairment of phonation or aphonia has resulted.
A novel form of treatment is paced glottic closure for controlling aspiration pneumonia.
Bilateral vocal fold paralysis
In the rare case of bilateral vocal fold paralysis, urgent tracheostomy may be necessary. Posterior laser cordotomy, arytenoidectomy, and suture lateralization of the arytenoid cartilage are three surgical options available to attempt decannulation. [4]
Dysphonia
Similar to other etiologies of dysphonia, patients presenting with stroke-related dysphonia may be treated conservatively or surgically. Nonsurgical modalities such as voice therapy predominate, with surgical intervention reserved only for the minority of patients who are appropriate candidates. Therapy focuses on strengthening the intrinsic laryngeal musculature and accessory muscles of respiration.
Patients who have had dysphonia due to vocal fold paralysis for less than 6 months are candidates for vocal fold injection thyroplasty (unless the nerve is known to have been cut, in which case medialization thyroplasty may be performed at any time).
Medialization thyroplasty and arytenoid repositioning procedures are indicated in patients whose paralysis lasts 12 months or more or for patients with no evidence of electrical recovery on electromyography (EMG) after 6 months.
Laryngeal Phylogeny
Phylogenetically, the primary function of the larynx is to prevent, via sphincteric control, aspiration of foreign material into the tracheobronchial tree. To do this, the human larynx contains 7 intrinsic adductors (compared with only 1 abductor) and 7 extrinsic laryngeal elevators (compared with only 4 depressors). Similarly, the airway protection functions of the larynx are involuntary, whereas the respiratory and phonatory functions are voluntary, albeit modulated by complex involuntary cortical feedback loops.
According to Negus, as early amphibians began to transition from an aquatic environment to land, increasing respiratory requirements favored the evolution of sphincter dilator muscles and cartilaginous structures to support them. [5] Endowed with both abductors and adductors, the larynx is able to close during swallowing, coughing, and tasks requiring increased intrathoracic pressure. Just as importantly, the larynx opens before respiration and subtly regulates the breathing cycle.
Despite the presence of the requisite functional elements, the primitive larynx provided no phonation. Negus described phonation as the least phylogenetically significant function, noting that, of all mammals, only humans have the ability to produce complex sounds. [5, 6] However, the human larynx has several anatomic characteristics that facilitate phonation at the expense of airway protection and respiratory regulation.
Laryngeal Anatomy and Embryology
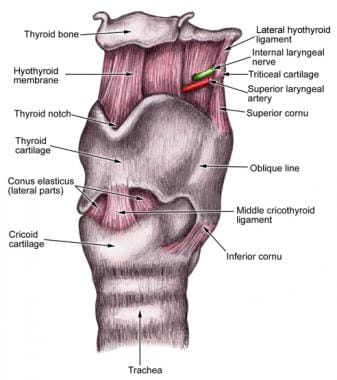
The larynx is a complex mucosal-lined structure composed of 9 distinct cartilage components connected by membranes, ligaments, and muscles, which separate the pharynx from the trachea (see the following images).
The larynx is derived from the fourth and sixth branchial arches. At the fourth week of fetal development, the laryngotracheal groove forms and subsequently invaginates to form the laryngotracheal diverticulum, thus dividing the primitive foregut into dorsal and ventral portions. Epithelial proliferation lateral to the laryngeal orifice then obliterates the lumen until recanalization occurs by the 10th week of gestation.
In contrast to the other branchial arch derivatives, the cartilages of the fourth and sixth arches develop from the lateral plate mesoderm rather than the neural crest of the midbrain and hindbrain. Development of the larynx begins during the fifth week of gestation, as mesodermal condensations called arytenoid swellings begin to form within the sixth arch. The arytenoid cartilage is formed by the seventh week of gestation, followed by the cuneiform and corniculate, at approximately the same time as the thyroid and cricoid cartilage.
In contrast to the early development of the remainder of the larynx, chondrification of the epiglottis, which develops at the location of the fourth arch, does not occur until the fifth month of gestation. The epiglottis may be derived from cells that have migrated to the location of the fourth arch from the hypobranchial eminence, although some investigators have reported mesodermal swellings within the arch that undergo chondrification after the remainder of the larynx does. The hyoid bone is derived from the second and third arches.
With the exception of the cricothyroid, which is derived from the fourth arch, the intrinsic musculature of the larynx is derived from the paraxial mesoderm of the first and second occipital somites (see the images below). Additional muscles involved in phonation and deglutition are derived from the first arch (mylohyoid, anterior belly of the digastric, tensor veli palatine), second arch (posterior belly of the digastric, stylohyoid), third arch (stylopharyngeus), and fourth arch (pharyngeal constrictors, levator veli palatine).



The superior laryngeal and recurrent laryngeal branches of the vagus nerve are derived from the fourth and sixth branchial arches, respectively.
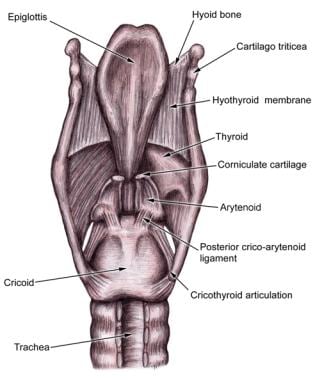
The epiglottis, thyroid cartilage, and cricoid cartilage are the 3 midline cartilaginous structures that make up the laryngeal framework (see the following images). Superiorly, the laryngeal framework is associated with the hyoid bone, which does not articulate with the larynx. Posteriorly, the paired arytenoid, corniculate, and cuneiform cartilages are supported by the midline cartilages. The arytenoid cartilages articulate inferiorly with the cricoid lamina, whereas the corniculate and cuneiform cartilages rest above the arytenoids, within the aryepiglottic fold.
Laryngeal motion
Motion of the larynx occurs via the cricothyroid and the cricoarytenoid synovial joints. The cricothyroid joint rotates along a common transverse axis between the inferior horns of the thyroid cartilage and the posterolateral aspect of the cricoid cartilage. The rocking motion of this joint changes the distance between the anterior aspect of the thyroid cartilage and the anterior cricoid cartilage, thereby stretching and adducting the vocal folds. The cricoarytenoid joint is located between the cricoid lamina and the broad base of the pyramidal-shaped arytenoid cartilage. This joint has 3 degrees of freedom, which include sliding (medially and laterally), rotating (medially and laterally), and tilting (anteriorly and posteriorly).
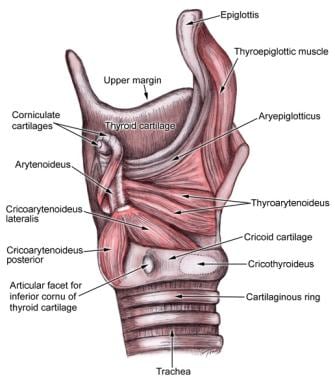
The functions of the intrinsic laryngeal musculature are summarized, as follows:
-
The posterior cricoarytenoid abducts the true vocal fold (TVF).
-
The cricothyroid stretches (lengthens) and adducts the TVF.
-
The lateral cricoarytenoid adducts the TVF.
-
The transverse arytenoids adduct the TVF.
-
The oblique arytenoids adduct the TVF.
-
The thyroarytenoid tightens the TVF.
-
The vocalis shortens the TVF.
The extrinsic suprahyoid muscles (stylohyoid, mylohyoid, geniohyoid, digastric) elevate the larynx. The extrinsic infrahyoid muscles (sternohyoid, sternothyroid, thyrohyoid, omohyoid) depress the larynx. See the image below.

Functional anatomy
The high position of the larynx in infants (and in many mammals) places the epiglottis in contact with the soft palate, affording some degree of separation between the airway and the digestive tract. By age 6 months, the human larynx has descended to its relatively low position. Despite this modification, both the epiglottis and the aryepiglottic folds continue to prevent the penetration of foreign material into the airway.
The true and false vocal folds function as paired one-way valves. The downward-turned false vocal folds, coupled with the air-trapping ventricles and saccules, prevent escape of air from the lower respiratory tract when adducted, while providing little resistance to inspired air. Conversely, the adducted true vocal folds have been shown to obstruct inhalation but not exhalation.
Neuroanatomy
Innervation of the larynx is provided by branches of the vagus nerve (cranial nerve [CN] X). The lower motor neurons reside within the nucleus ambiguous of the medulla. Cell bodies of the sensory nerves reside within the rostral nodose ganglion, with central connections to the nucleus tractus solitarius. Some authors propose additional vagal central sensory connections with the spinal trigeminal nucleus, cuneate nucleus, and the dorsal horn of the C1 and C2 cord segments. [7]
The superior laryngeal nerve (SLN) branches from the vagus just below the nodose ganglion and then divides into separate motor and sensory branches. The internal branch traverses the thyrohyoid membrane and provides sensation to the laryngeal surface of the epiglottis and to the larynx. The basic arrangement of the sensory innervation of the SLN is that the anterior branches innervate the laryngeal surface of the epiglottis; the middle branches, the supraglottis above the vestibule; and the posterior branches, the posterior arytenoid/hypopharynx/caudal vocal fold. The external branch descends with the inferior constrictor to provide motor innervation to the cricothyroid muscle.
The recurrent laryngeal nerve (RLN) provides both sensory and motor innervation to the larynx. This nerve branches from the vagus below the subclavian artery on the right and the ligamentum arteriosum on the left. It then ascends within the tracheoesophageal groove and enters the larynx adjacent to the cricothyroid articulation. The motor fibers innervate the ipsilateral intrinsic laryngeal musculature, with the exception of the interarytenoid muscles, which receive bilateral innervation. The RLN provides sensation to the true vocal folds and the subglottis, although Galen anastomosis of the RLN and the SLN at the level of the anterior subglottis is well described. [8]
The region of the supraglottis contains the highest density of sensory fibers, with the posterior aspect containing more sensory receptors than the anterior glottis. Diverse laryngeal sensory receptors, including chemoreceptors, mechanoreceptors, and paraganglia, have been described throughout the larynx. Chemoreceptors, specifically those that detect decreased chloride concentrations (water, gastric fluid, and saliva), have been shown to stimulate reflexes, resulting in apnea, bradycardia, hypertension, and increased systemic vascular resistance in newborn animals. [9] These reflexes gradually disappear as the central nervous system (CNS) matures. A wide variety of mechanoreceptors, including touch, proprioception, flow, pressure, and articular joint receptors, have also been described. [10]
Neurophysiology
Microstimulation studies in animals have established the location of the laryngeal motor cortex. The laryngeal motor cortex overlaps the lower lateral face portion of the motor cortex. [11] Stimulation of the motor cortex produces bilateral adductor activity coupled with abductor inhibition. Recent functional MRI studies have suggested that there is a common motor region underlying adduction/abduction and tensing/relaxing of the vocal folds. This motor region was a ventromedial peak located deep in the central sulcus that corresponds with Brodmann area 4p and a dorsolateral peak located in area 6, which is more superficial. The motor cortex also appears to in a dorsal position directly adjacent to the lip area. [12]
Most evidence suggests multiple cortical, subcortical, midbrain, and brainstem connections between the motor cortex and the nucleus ambiguous. Stimulation of these subcortical regions produces nonverbal phonation associated with states of emotional arousal. The periaqueductal gray matter plays an especially important role in the coordination of cortical and subcortical inputs, with complete mutism resulting from ablative lesions in this region. Although the dominant hemisphere is responsible for speech production, the nondominant hemisphere modulates the inflection, intonation, and timing of speech. The cerebellum may also have a modulatory role.
The nucleus ambiguus has a rostral-to-caudal arrangement of lower motor neurons. The cricothyroid is innervated by the most rostral neurons, followed by the thyroarytenoid, the lateral cricoarytenoid, and the transverse/oblique arytenoids. Lower motor neurons that innervate the single abductor, the posterior cricoarytenoid, are located ventrally to the adductor motor neuron pool. Some authors interpret this arrangement to reflect the preferential connections between the adductor and abductor lower motor neurons with the periaqueductal gray matter and the inspiratory centers of the medial reticular formation, respectively. [13]
Laryngeal dysfunction in stroke
Primary dysfunction of the larynx following stroke is most frequently the result of an insult to the nucleus ambiguous and the nucleus solitarius; however, some authors have described insults to the cortical and subcortical pathways that result in loss of the laryngeal cough reflex. [14] Patients with hemispheric stroke exhibit signs of laryngeal dysfunction. Many of these patients have delayed laryngeal elevation and delayed laryngeal closure, compromising airway protection. [15] Infarction of the nucleus ambiguous is usually related to occlusion of the posterior inferior cerebellar artery (PICA), which results in lateral medullary infarction (Wallenberg syndrome). Infarction of the cortical and subcortical motor and sensory pathways may result in vocal fold incoordination rather than frank paresis or paralysis. [16]
Upper motor neuron laryngeal manifestations include spastic paresis and decreased agility (cerebrum); resting tremor, dystonia, and rigidity (basal ganglia); and intention tremor and dysdiadokinesis (cerebellum). Lower motor neuron laryngeal manifestations include atrophy and flaccid paresis or paralysis.
Laryngeal manifestations of stroke play a significant role in the morbidity and mortality of stroke, via both direct and indirect mechanisms (see the table below). Therefore, the otolaryngologist is an important contributor to the multidisciplinary team of specialists required to successfully manage the sequelae of stroke in both the short- and long-term rehabilitative stages of treatment.
Table 1. The Direct and Indirect Effects of Stroke and the Treatment of Stroke Symptoms in the Larynx (Open Table in a new window)
Function |
Deficit |
Direct |
Indirect |
Airway protection |
Aspiration |
Pneumonia |
Laryngopharyngeal reflux, sinusitis secondary to nasogastric tube feeding |
Respiration |
Vocal cord paresis or paralysis |
Respiratory failure |
Complications of tracheostomy |
Phonation |
Vocal cord paresis or paralysis |
Dysphonia or aphonia |
Exacerbation of associated communication deficits |
Laryngeal Evaluation Following Stroke
According to the Neurolaryngology Committee of the American Academy of Otolaryngology – Head and Neck Surgery (AAO-HNS), the evaluation of patients with laryngeal symptoms should include a history, voice evaluation, neurolaryngologic evaluation, and stroboscopic evaluation. The recommendations in this section are based on a report by the Neurolaryngology Committee of the AAO-HNS. [17]
History
The following information should be elicited from the patient:
-
Onset of symptoms (sudden vs progressive)
-
Aggravating or alleviating factors (eg, speaking, singing, stress, prolonged phonation)
-
Associated symptoms (eg, odynophonia, dysphagia, other neurologic symptoms, systemic disease)
-
Character – Voice quality (eg, raspiness, breathiness, strain), flow (eg, decreased breath support, projection, or volume)
-
Control
-
Vocal fatigue (eg, decreased range, pitch control, or voice breaks)
Voice evaluation
The patient’s voice should be assessed while he or she is counting and reading a passage of balanced vowels and consonants, such as the "Rainbow passage" (balanced consonants and vowels) or the Marvin Williams passage (includes all voiced sounds). Attention should be paid to the voice’s fluidity (fluid or nonfluid), articulation (clear or indistinct), and the voice quality (normal or raspy, breathy, strained, hypernasal, hyponasal). Depending on the location, acuity, and severity of the stroke, every parameter of voice characteristics may or may not be affected.
The Rainbow passage follows:
When the sunlight strikes raindrops in the air, they act like a prism and form a rainbow. The rainbow is a division of white light into many beautiful colors. These take the shape of a long round arch, with its path high above, and its two ends apparently beyond the horizon. There is, according to legend, a boiling pot of gold at one end. People look, but no one ever finds it. When a man looks for something beyond his reach, his friends say he is looking for the pot of gold at the end of the rainbow.
The Marvin Williams passage follows:
Marvin Williams is only nine. Marvin lives with his mother on Monroe Avenue in Vernon Valley. Marvin loves all movies, even eerie ones with evil villains in them. Whenever a new movie is in the area, Marvin is usually an early arrival. Nearly every evening Marvin is in row one, along the aisle.
Neurolaryngeal evaluation
Flexible laryngoscopy should be performed while the patient is at rest and during phonation. Before evaluation of the larynx, velopharyngeal function should be visualized with nasopharyngeal endoscopy. Symmetrical elevation of the palate and closure against the posterior pharyngeal wall should be observed. With the patient breathing comfortably, the resting tone and position of the vocal folds should be noted. Any mucosal lesions should be identified, and special attention should be paid to retained secretions or food within the pharynx, because these can be important signs of pharyngeal weakness and a risk for dysphagia. [18, 19, 20, 21]
Involuntary motion of the vocal folds, including tremor, myoclonus, and spasm, should be identified. Laryngeal tremor is characterized by involuntary rhythmic movements of the vocal folds during rest and during phonation (see Laryngeal Tremor).
In contrast to tremor, myoclonus is characterized by the abrupt, nonrhythmic nature of the movements, although slow (4-6 Hz) rhythmic movements may also be observed. Laryngeal myoclonus may be accompanied by myoclonus of other neck structures, referred to as branchial or oculopalatal myoclonus. The pathophysiology of this movement disorder has been localized to the dento-olivary pathway.
Laryngoscopy performed during phonation enables the assessment of laryngeal mobility. Both adductor and abductor function should be systematically evaluated. Abduction may be tested by having the patient repeatedly sniff through the nose, and adduction may be evaluated by having the patient phonate the sound /i/. The vocal folds should move symmetrically and quickly. Unilateral weakness suggests a lower motor neuron lesion, whereas global weakness suggests upper motor neuron dysfunction. Motion-induced movement disorders (laryngeal dystonia) may also be observed. [22]
Poststroke Dysphagia and Aspiration
Dysphagia and aspiration are factors that significantly affect the morbidity, mortality, and cost of care for patients who have experienced a stroke. [18, 19, 20, 21, 23] Patients with laryngeal manifestations of stroke may have decreased sensation, impaired motor function, and decreased laryngeal cough reflex. Comorbid deficits in tongue, pharyngeal, and esophageal function further increase the risk of aspiration.
A questionnaire survey conducted in Japan, by Ikeda et al, found dysphagia to be the second most common stroke complication (29.3% of respondents), after dementia (30.9%). Moreover, dysphagia was considered to be the most difficult complication to treat (40.4%), with 25.3% of respondents indicating that a lack of clinical evidence exists for dysphagia therapy. [24]
Videofluoroscopic evaluation of patients who have had an acute stroke has revealed aspiration in 20-70% of patients. [18] Dysphagia, sedative medications, and witnessed aspiration are associated with the development of pneumonia. Aspiration pneumonia has an estimated mortality of 20-65%. [6] The early treatment of patients with dysphagia via a multidisciplinary approach that includes a speech-language pathologist is associated with improved outcomes.
The posteroinferior displacement of the epiglottis, adduction of the false vocal folds, and adduction of the true vocal folds are 3 functional barriers to aspiration of solid and liquid boluses. In addition, the elevation and anterior displacement of the larynx by the extrinsic laryngeal musculature, as well as the stiffening of the aryepiglottic folds during the pharyngeal phase of swallowing, further protects the airway from inadvertent aspiration of food products into the tracheobronchial tree. These laryngeal movements must be synchronized with the reflexive pharyngeal components of swallowing (ie, velopharyngeal closure, constriction of the pharynx, posterior displacement of the tongue base, relaxation of the upper esophageal sphincter). The dysregulation of any component of the pharyngeal phase of swallowing may increase the aspiration risk, because the human larynx has evolved to favor phonation at the expense of airway protection. [22]
The terms penetration and aspiration are used to describe varying degrees of abnormal entrance of material into the larynx and below. [25] Penetration occurs when material enters the larynx to the level of the true vocal folds, and aspiration refers to material that descends past the true vocal folds into the trachea. When foreign material enters the larynx, the activation of supraglottic chemoreceptors stimulates a cough reflex via the superior laryngeal nerve. Reflexive cough has a sensitivity of 24-48% as an indicator of aspiration, as diagnosed with videofluoroscopic swallow evaluation. [19] However, sensory denervation of the larynx and trachea may allow silent aspiration to occur. In fact, silent aspiration occurs in 2-25% of acute stroke patients. [18, 20]
A study by Onofri et al indicated that impairment of laryngeal sensitivity following stroke is an important factor in laryngeal penetration and tracheal aspiration of food after swallowing. The study involved 91 patients with ischemic stroke who were experiencing oropharyngeal dysphagia (average poststroke period 22.6 months). An association between impaired laryngeal sensitivity and laryngeal penetration and tracheal aspiration was found for all three food consistencies used in the report (purée, thickened liquid, and liquid). [26]
In a prospective cohort study, Zhang et al reported that following acute ischemic stroke, reduced laryngeal elevation velocity prior to closure of the vestibule independently predicts aspiration. [27]
A study by Kojima et al indicated that in patients with poststroke dysphagia, the presence of cognitive dysfunction and a reduction in activities of daily living increase the risk that the dysphagia will not improve. The study, which included 123 patients, reported that in terms of predicting nonimprovement of dysphagia, the presence of both stroke and cognitive dysfunction had a sensitivity and specificity of 75.9% and 78.3%, respectively, and the presence of both stroke and disuse syndrome had a sensitivity and specificity of 66.0% and 71.4%, respectively. [28]
A report by Castagna et al derived similar results, with the study indicating that in older patients who have suffered an acute neurologic event, those with, on admission to neurorehabilitation, poor functional conditions and cognitive impairment tend to have worse outcomes, at discharge, with regard to dysphagia. [29]
Assessing aspiration risk
A study by Feng et al of 1220 stroke patients found that in those with dysphagia, the risk of developing aspiration pneumonia within 1 year poststroke was 4.69 times higher than in patients without dysphagia. Moreover, patients with dysphagia had a significantly greater 5-year mortality rate, the adjusted hazard ratio being 1.84. [30]
Clinical swallowing examination (CSE), cough reflex testing, fiberoptic endoscopic evaluation of swallowing (FEES), [2] and videofluoroscopic swallow evaluation (VSE) are tools that are available for assessing aspiration risk.
CSE typically consists of identifying risk factors for aspiration (ie, dysphonia, dysarthria, abnormal gag reflex, abnormal volitional cough, cough after swallow, voice change after swallow). Cough reflex testing uses aerosolized or nebulized tussigenic compounds to stimulate a reflexive cough.
FEES consists of endoscopic examination of the pharynx and larynx during administration of liquid, puree, and solid-food boluses dyed with food coloring to enhance visualization. The endoscopist notes evidence of penetration and aspiration. Similarly, VSE enables visualization of penetration and aspiration based on real-time radiographic imaging of the pharynx and larynx during swallowing attempts with liquids and solids of varying consistency.
Evidence-based evaluation recommendations
CSE is less sensitive and specific than instrumental evaluations in patients with silent aspiration. However, CSE remains a reliable, timely, and cost-effective screening examination. Some of the evidence-based clinical practice guidelines of the American College of Chest Physicians (ACCP) for the evaluation of cough and aspiration due to oral-pharyngeal dysphagia are as follows:
-
Patients with cough, pneumonia, or both and conditions that place them at high risk for aspiration should be referred for CSE.
-
Self-reported and family-reported symptoms of dysphagia should be evaluated with CSE.
-
Volitional cough is not a reliable marker of aspiration.
-
Reflexive cough and volitional cough have not been validated as reliable risks of aspiration.
-
Patients with dysphagia should undergo FEES or VSE.
-
FEES and VSE are useful for determining compensatory strategies for safe swallowing.
The ACCP, American Gastroenterological Association (AGA), and the American Speech Language and Hearing Association (ASHA) uniformly advocate a multidisciplinary approach to dysphagia. The US Agency for Healthcare Research and Quality (AHRQ) has reported that screening programs for patients who have experienced acute stroke followed by referrals to dysphagia specialists dramatically reduces the rate of aspiration pneumonia.
Medical management of dysphagia
Management approaches depend on the degree of dysphagia and the comorbid conditions. [31] The risk of aspiration has been demonstrated to decrease with time after stroke. To meet short-term nutritional requirements in patients with significantly decreased mental status or severe dysphagia, nasogastric tube feeding may be indicated. Epistaxis and increased gastroesophageal or laryngopharyngeal reflux should be kept in mind as possible complications of this therapy. For long-term, nonoral feeding, a gastrostomy tube should be considered.
In patients with dysphagia and intact mental status, dysphagia therapy focuses on techniques to minimize aspiration by increasing anterior laryngeal excursion, the opening of the upper esophageal sphincter, and the pharyngeal clearance. Use of postural maneuvers, different delivery methods (spoon vs cup vs straw), and the alteration of food consistency are other components of dysphagia therapy that may reduce or eliminate aspiration. Targeted physiologic swallowing exercise programs, electromyographic biofeedback, and electrical stimulation of the extrinsic laryngeal muscles have also been shown to reduce aspiration in small studies. [32, 33] Use of angiotensin-converting enzyme inhibitors to reduce aspiration via a substance P–mediated mechanism has been described, [34] although correlation with FEES or VSE has not been performed.
Surgical management of dysphagia
Surgical intervention is indicated in a small minority of patients with dysphagia. Surgical interventions such as total laryngectomy, supracricoid partial laryngectomy with cricohyoidoepiglottopexy, tracheoesophageal diversion techniques, various types of supraglottoplasty, and tracheostomy with cuffed tracheostomy tube have been described in patients with intractable aspiration, although significant impairment of phonation or aphonia has resulted. [3] Medialization thyroplasty has been advocated for isolated laryngeal incompetence (ie, vocal fold paralysis without sensory deficit or discoordination of the swallow reflex), although the effect of this procedure on swallowing function has not been studied well. [35]
A novel form of treatment is paced glottic closure for controlling aspiration pneumonia. This involves surgical placement of a stimulator on the ipsilateral recurrent laryngeal nerve. Pulses effect closure of the glottis for airway protection. One small study showed statistically significant improvement in vocal fold adduction and decreased rates of pneumonia in two of three patients with brainstem/basal ganglia/cerebellar stroke who received paced glottic closure treatment. [36] While these results are promising, further clinical evidence is needed prior to widespread adoption.
A promising approach to stroke-induced dysphagia that merits further investigation is the use of repetitive transcranial magnetic stimulation (rTMS). This modality has been found to be more effective than transcranial direct current stimulation, particularly for patients with non-hemorrhagic cerebral infarction. In a controlled trial, Jiao et al found that rTMS of pharyngeal constrictors significantly improved swallow function. [37] Park et al reported that rTMS of the mylohyoid similarly improved swallow function in post-stroke patients. [38] A meta-analysis indicated that rTMS is most effective in the acute phase of stroke and in patients with targeted brainstem injuries. [39] The most effective therapeutic protocol for rTMS remains a source of investigation.
It is important to note that stroke not only alters laryngeal function but may also affect velopharyngeal closure, upper esophageal sphincter relaxation, and pharyngeal constrictor function. Therefore, direct interventions that only target laryngeal function may have limited efficacy.
For a more comprehensive review of the surgical treatment of chronic aspiration and dysphagia please see the article entitled Surgical Management of Chronic Aspiration.
Poststroke Vocal Fold Paresis or Paralysis
The accepted terminology for impairment of vocal fold mobility is vocal fold immobility, which is applied until the specific etiology (neurologic vs mechanical) of the impairment is elucidated. In the setting of stroke, prolonged intubation and other iatrogenic injuries should also be considered as possible causes. The term paralysis refers to nonmobile vocal folds with minimal-to-no neural signal transmission, whereas paresis refers to vocal folds with partial mobility and reduced neural signal transmission. [40]
Cerebrovascular accident (CVA) is an uncommon cause of vocal fold paralysis. In this setting, vocal fold paralysis is usually associated with a brainstem stroke, or lateral medullary syndrome (Wallenberg syndrome), which is characterized by severe pharyngeal dysphagia, palatal incompetence, vertigo, facial pain, and Horner syndrome. [41] The position of the paralyzed vocal fold was once thought to be related to the prognosis for recovery (Semon law); however, later evidence supports the concept that vocal fold position is not correlated with the either the location of vagal injury or the likelihood of clinical improvement. [3]
Using the National (Nationwide) Inpatient Sample (2000-2019), Vasan et al found that out of over 12.4 million hospital patients with stroke, 0.1% of those with acute ischemic stroke and 0.1% of those with intracerebral hemorrhage suffered vocal fold paralysis. Over the two-decade period of the sample, the investigators noted an increase in the overall number of ischemic stroke patients with vocal fold paralysis, with the percentage fluctuating between 0.8% and 0.15%. Over the same period, the number of patients with intracerebral hemorrhage who had vocal fold paralysis also increased. [42]
Vocal cord assessment
Patients who develop unilateral vocal fold paresis may be asymptomatic if the vocal fold is in the median or paramedian position. Paralysis with lateral vocal fold position manifests primarily in aspiration and dysphonia.
Evaluation of immobile vocal folds typically includes flexible fiberoptic laryngoscopy and computed tomography (CT) scanning or magnetic resonance imaging (MRI) of the complete course of the recurrent laryngeal nerves; it may also include direct laryngoscopy and palpation of the cricoarytenoid joints, as well as laryngeal electromyography (LEMG). Common examination findings in vocal fold paralysis include vocal fold atrophy and anteromedial displacement of the affected arytenoid cartilage, with subsequent foreshortening and inferior displacement of the true vocal fold.
Chevalier described lateral displacement of the affected arytenoid cartilage by the mobile arytenoid cartilage ("jostle sign"). Hyperadduction of the mobile hemilarynx may represent another compensatory response. Maximum phonation time (MPT) using the voiced vowel /i/ should be assessed. The normal MPT is greater than 21 seconds. In patients who undergo medialization thyroplasty, MPT is a useful benchmark to compare preoperative and postoperative laryngeal function. [35]
Management
In the rare case of bilateral vocal fold paralysis, urgent tracheostomy may be necessary. Posterior laser cordotomy, arytenoidectomy, and suture lateralization of the arytenoid cartilage are 3 surgical options available to attempt decannulation. [4] Each of these procedures is used in an attempt to provide an adequate posterior glottic airway, with continued anterior glottic closure for phonation.
Prognosis
Recovery from vascular insult to the motor innervation of the larynx is similar to that of other CVA motor deficits (ie, earlier improvement portends a more rapid and complete recovery). Clinical consequences of vocal fold paralysis may range from none (asymptomatic) to airway obstruction that requires urgent tracheostomy.
The reader is referred to the excellent text edited by Sulica and Blitzer for further discussion of vocal fold paralysis. [40]
Poststroke Dysphonia
Additional testing may be warranted in patients who experience significant dysphonia as a sequela of stroke. In fact, because supranuclear lesions may result in dysphonia without obvious vocal fold paralysis, additional testing modalities are necessary for proper diagnosis. Although dysphonia must be differentiated from pure dysarthria, aphasia, or dyspraxia, phonatory dysfunction (frequently resulting from presbylarynx) is very common as a comorbid condition in patients with dysarthria. Dysphonia, therefore, plays an additive role in the communication impairment of patients who have experienced stroke.
Assessment of dysphonia
Videostroboscopy is a critical component of the evaluation in patients with dysphonia. Stroboscopic visualization of the larynx during phonatory tasks provides a representation of the mucosal wave as well as a high resolution image of the laryngeal architecture. The videostroboscopic examination should include visualization of the larynx during inhalation, cough, sustained vowel (/i/), and sustained vowel with varying degrees of loudness. Both structural and functional abnormalities are assessed during review on permanent media after recording. Go to Stroboscopy for a detailed discussion of this important diagnostic tool.
Additional laryngeal analysis, including acoustic, aerodynamic analysis, high-speed digital imaging, and kymography may be indicated in certain cases.
A retrospective study by Kim et al indicated that in patients with ischemic stroke who suffer from associated dysphonia, nutritional biomarker levels may correlate with the degree of dysphonia. According to the investigators, multiple linear regression analysis revealed that in study patients, lower serum levels of transferrin and prealbumin predicted a worse dysphonia severity index (DSI) score, while lower prealbumin alone predicted a lower maximum phonation time (MPT). The report suggested that the relationship between the biomarkers and dysphonia may be associated with the detrimental effect of malnutrition on muscles (and therefore, vocal fold muscles). [43]
Management of dysphonia
Similar to other etiologies of dysphonia, patients presenting with stroke-related dysphonia may be treated conservatively or surgically. Nonsurgical modalities such as voice therapy predominate, with surgical intervention reserved only for the minority of patients who are appropriate candidates. Therapy focuses on strengthening the intrinsic laryngeal musculature and accessory muscles of respiration. A pilot study found that combined respiratory muscle therapy improved patients' perception of voice function, spirometry parameters, several acoustic parameters (including maximum phonation time), and total semitone range. [44]
Patients who have had dysphonia due to vocal fold paralysis for less than 6 months are candidates for vocal fold injection thyroplasty (unless the nerve is known to have been cut, in which case medialization thyroplasty may be performed at any time). Historically, many materials, including fat, Teflon, Gelfoam, calcium hydroxylapatite, collagen, and hyaluronic acid, have been used as injection material. Teflon has fallen out of favor because of granuloma formation and is no longer available. All of these materials (except calcium hydroxylapatite) undergo resorption and therefore require initial overinjection.
Medialization thyroplasty and arytenoid repositioning procedures are indicated in patients whose paralysis lasts 12 months or more or for patients with no evidence of electrical recovery on electromyography (EMG) after 6 months. Go to Unilateral Vocal Fold Paralysis for more detailed information on these procedures.
Prognosis
In patients with significant dysphonia 6-12 months after the onset of symptoms, the prognosis for spontaneous recovery is poor. Although function improves in many patients with idiopathic vocal fold paralysis, the immobile vocal fold only rarely recovers mobility. Although laryngeal electromyography (LEMG) is the best tool for predicting return of vocal fold function, accurate prediction of return of function ranges from 13% to 80%. A working group of neurolaryngologists convened to provide a consensus statement regarding the role of LEMG. [45]
-
Illustration of the larynx.
-
Illustration of the glottic and supraglottic larynx.
-
Illustration of the larynx, posterior view.
-
Illustration of the larynx, nasopharyngeal view.
-
Illustration of the intrinsic muscles of the larynx, sagittal view.
-
Illustration of the intrinsic muscles of the larynx, sagittal view.
-
Illustration of the extrinsic muscle insertions of the larynx.
-
Illustration of the intrinsic muscles of the larynx, superior view.
-
Illustration of the intrinsic muscles of the larynx.
Tables
Function |
Deficit |
Direct |
Indirect |
Airway protection |
Aspiration |
Pneumonia |
Laryngopharyngeal reflux, sinusitis secondary to nasogastric tube feeding |
Respiration |
Vocal cord paresis or paralysis |
Respiratory failure |
Complications of tracheostomy |
Phonation |
Vocal cord paresis or paralysis |
Dysphonia or aphonia |
Exacerbation of associated communication deficits |






