
Are Plants Used as a Combating Strategy against Tuberculosis in the Mpumalanga Province, South Africa?


Department of Chemistry, Cape Peninsula University of Technology, Symphony Road, Bellville Campus, Bellville 7535, South Africa
*
Authors to whom correspondence should be addressed.
Appl. Sci. 2023, 13(8), 5008; https://doi.org/10.3390/app13085008
Submission received: 20 March 2023
/
Revised: 3 April 2023
/
Accepted: 14 April 2023
/
Published: 16 April 2023
(This article belongs to the Special Issue Chemical and Functional Properties of Food and Natural Products)
Abstract
:The burden of tuberculosis (TB) disease is a global health challenge accounting for thousands of deaths. TB is unevenly distributed in South Africa, with some provinces having more than 70% of the TB burden. In Mpumalanga Province, TB is ranked as the sixth leading cause of death. Antituberculosis agents are usually costly, with numerous unwanted side effects. This has prompted the major use of herbs which have an imperative biological role against tuberculosis and are easily accessible. A comprehensive review of plants used as a combating strategy against tuberculosis in Mpumalanga Province was conducted. An in-depth literature search was performed using scientific databases, theses, dissertations and ethnobotanical books. Twenty-four (24) plant species were reported by the people of Mpumalanga for the treatment of tuberculosis. Fifteen (15) plant species have been investigated for antituberculosis activities, and seven antimycobacterial compounds were successfully isolated. This review validates the use of plants against tuberculosis in Mpumalanga Province and, thus, identified species that may be explored for further scientific studies.
1. Introduction
Tuberculosis (TB) is a multisystemic infectious bacterial disease caused by Mycobacterium tuberculosis, a rod-shaped bacterium [1]. It is a deadly transmissible disease that affects almost any body part, but it is primarily an infection of the lungs. TB occurs when an individual breathes in TB bacteria (M. tuberculosis). The bacteria can settle in the lungs and then begin to grow, thereby moving through the blood and to other parts of the body. The disease attacks persons of all ages, including babies, preschool children, and the elderly as they have a declining immune system compared to healthy adults. A person only needs to breathe in a few germs to become infected. TB disease can be easily spread in overcrowded settings and in conditions of malnutrition and poverty [2].
TB transmission occurs when a person inhales droplet nuclei (about 1–5 microns in diameter) containing M. tuberculosis (also called tubercle bacilli), and the droplet nuclei traverse the mouth or nasal passages, upper respiratory tract, and bronchi to reach the alveoli of the lungs [3]. A number of tubercle bacilli enter the bloodstream and start spreading throughout the body. The tubercle bacilli can reach any part of the body (such as the brain, larynx, lymph node, spine and bones) [3]. If the immune system becomes too weak to keep the tubercle bacilli under control or fails to stop the bacilli from growing, the bacilli begin to multiply rapidly.
TB symptoms are very variable, and they depend on the part of the body which has been infected. For example, if TB spreads to the lymph nodes, it may cause swollen glands at the sides of the neck or below the arms. In some other cases, some people are infected with the TB bacteria, but do not experience any significant symptoms, and this condition is known as latent TB [4]. This condition can stay dormant for years before developing into active TB disease. Generally, active TB disease symptoms (Figure 1) include chest pain, coughing of blood, fever, loss of appetite, night sweats and weight loss, and chills [1,4]. If not treated, complications such as liver or kidney problems, heart disorders, and fluid collection between the lungs frequently occur resulting in shortness of breath [5].
1.1. Tuberculosis: A Global Pandemic
TB is a global disease, found in every country. It is one of the top 10 leading causes of death and one of the most burden-inflicting diseases in the world [1]. In 1993, the World Health Organization (WHO) proclaimed TB as a global pandemic and urged coordinated efforts by all countries to prevent millions of deaths caused by this disease in the coming years [6]. In 2021, a report revealed by the WHO also showed that approximately 10.6 million people (accounting for 6 million men, 3.4 million women, and 1.2 million children) fell sick with TB, and even though it is a preventable and curable disease, about 1.5 million people died from this disease (including 187,000 people with HIV) worldwide, thereby making it the world’s second-most infectious killer after COVID-19 [7]. Recently, new TB cases have been reported to occur in thirty (30) high TB burden countries. Out of these 30 burden countries, eight countries accounted for two-thirds (2/3) of the new TB cases with India leading the list, followed by China, Indonesia, Philippines, Pakistan, Nigeria, Bangladesh and South Africa [7]. Although progress is being made in reducing the incidence of TB cases, it has been very slow, and it is projected that the world will not eliminate TB as a global public health threat by 2035 as envisaged. South Africa has been reported as one of the 30 high-TB-burden countries which account for a total of 87% of the estimated incident cases globally; South Africa accounts for 3% of TB cases worldwide [8]. This high rate of TB cases in South Africa has been fueled since the early 1990s by the HIV/AIDS epidemic that has negatively affected the country’s TB control [8].
Tuberculosis is unevenly dispersed in South Africa, with some provinces having more than 70% of the TB burden. Mpumalanga has reported increasing numbers of positive cases of TB since 2018 [9]. This plague has deprived many families of their loved ones, communities of their leaders, and the province of its future. Recently, the province was ranked sixth with a high incidence rate of TB (402 per 100,000) in South Africa [8]. In addition, Mpumalanga was also recently identified as one of the provinces with the highest rate of TB that is resistant to rifampin (a drug used for the treatment of TB) [10]. This incidence of TB in the province is large because of unemployment, poverty, migration, a high rate of population growth, and HIV/AIDS [11]. Thus, there is a need for effective strategies to control and manage this disease.
1.2. Anti-Tuberculosis Agents and Their Potential Side Effects
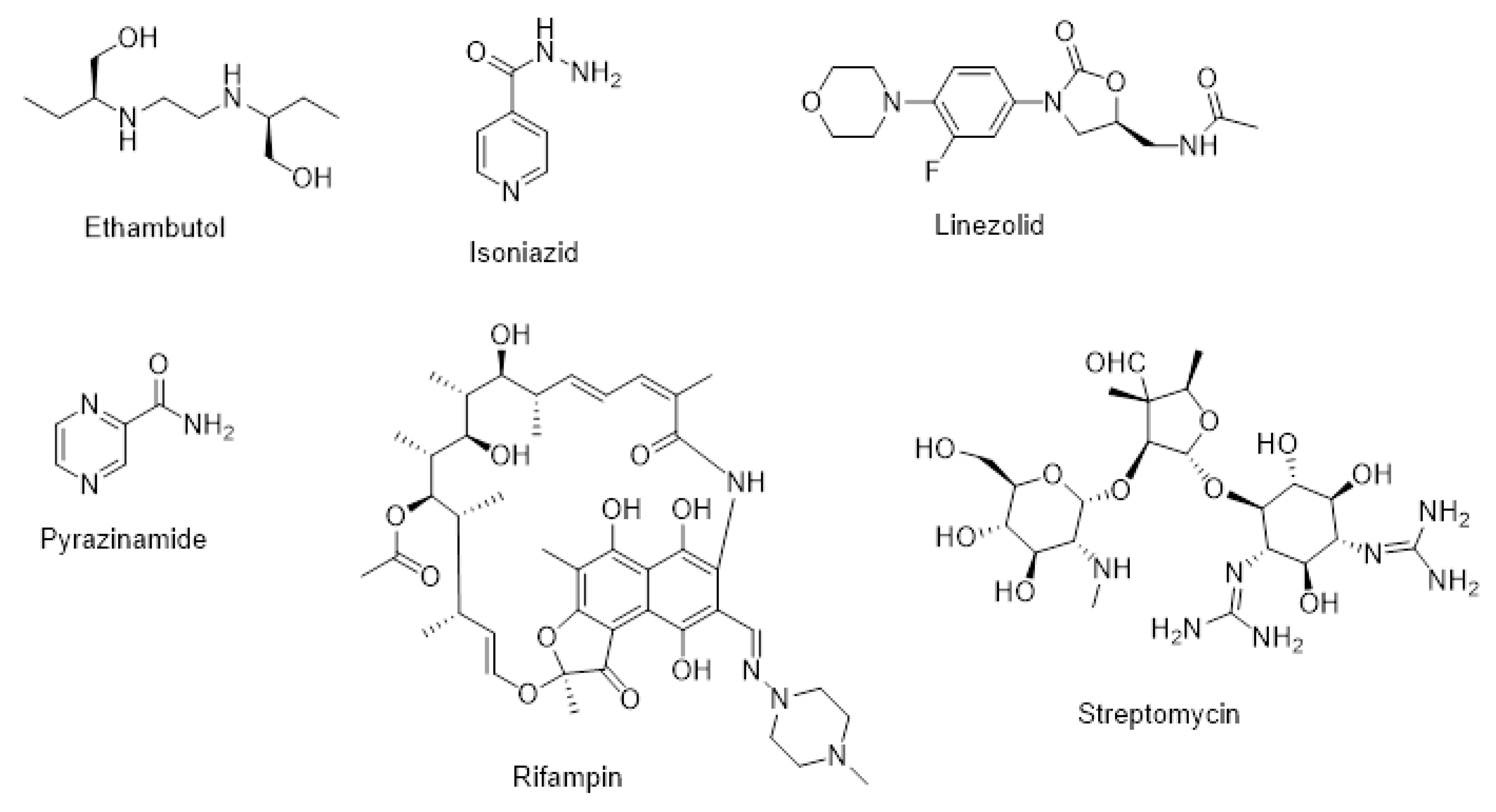
There have been numerous anti-tuberculosis drugs or agents (Table 1) used to treat TB. The most common drugs are ethambutol, Isoniazid, linezolid, pyrazinamide, rifampin, and streptomycin (Figure 2). A comprehensive description of these antituberculosis agents together with their potential side effects is given below.
Ethambutol, an essential first-line antituberculosis drug, possesses bacteriostatic action against Mycobacterium tuberculosis [12]. It is also used as part of a combination regimen to treat non-tuberculous mycobacterial infections [13]. This medication works by blocking the bacteria that cause TB from growing or increasing in number [13]. Although the exact mechanism of action of ethambutol is not fully known, evidence suggests that ethambutol performs its bacteriostatic activity against TB bacilli by exhibiting inhibition against arabinosyl [13]. Disruption of arabinogalactan formation inhibits the synthesis of the mycolic-arabinogalactan–peptidoglycan complex, thereby leading to increased permeability of the cell wall. However, several reports have indicated that ethambutol causes serious side effects that can reduce its usage for the treatment of TB. Some of the most common side effects of the drug include vomiting, swelling of the face, blurred vision, rash, breathlessness and nausea [14].
Isoniazid is one of the more potent antimicrobial agents mostly used to treat tuberculosis. It is used to treat both active and latent TB. This drug was recommended in 1963 for use as monotherapy in the deterrence of activation of tuberculosis in patients suffering from latent tuberculosis [15]. It is listed as one of the vital medicines for the treatment of TB in the WHO’s list of essential medicines. Isoniazid works by inhibiting the lipid and DNA synthesis of M. tuberculosis, thereby resulting in the inhibition of cell wall formation and development [16]. However, this drug is frequently used together with other antituberculosis agents such as rifampicin, pyrazinamide, and either streptomycin or ethambutol. The common side effects of isoniazid include liver inflammation, numbness in the hand and feet, liver failure and increased blood levels of liver enzymes [17].
Linezolid is the first in a new class of oxazolidinone antibiotic drugs used to treat various types of infections, including drug-resistant TB [18]. It is among the list of essential drugs recommended by WHO against the activity of M. tuberculosis [19]. Linezolid works by disrupting bacterial growth, thereby inhibiting bacterial protein production [20]. This mechanism of action is unique in that it prevents the start of bacterial protein synthesis. Despite the effectiveness of this drug in the treatment of TB, safety is one of the key concerns. Some of the potential side effects of linezolid are headache, nausea, difficulty breathing, swelling in your face or throat, discoloration of the tongue and diarrhea [21]
Pyrazinamide is another anti-tuberculosis agent that is structurally related to nicotinamide and very effective against M. tuberculosis and other mycobacterium strains [22]. Recently, pyrazinamide was reinstated as first-line therapy to solve challenges related to resistant strains as the incidence of tuberculosis is surging [23]. Though the mechanism of action of pyrazinamide is not fully known, its structure is similar to that of nicotinamide, and so it is assumed that pyrazinamide intervenes with the nucleic acid metabolism of bacterial cells. However, one of the major therapeutic limitations of the use of pyrazinamide is hepatoxicity [23]. Other limitations include gastrointestinal upset, and skin rashes can be associated with pyrazinamide administration [24]. In addition, the use of pyrazinamide treatment has also been linked to liver injury, notably resulting in a hepatitis-like liver injury in a patient suffering from tuberculosis [25,26].
Rifampin, also commonly known as rifampicin, is an antibiotic used for the treatment of various types of mycobacterial infections and in combination with other antituberculosis agents (ethambutol, isoniazid, and pyrazinamide) to treat active or latent TB [27]. It has a wide-ranging antibacterial spectrum, including activity against numerous forms of Mycobacterium. It works by inhibiting the bacterial DNA-dependent RNA polymerase, thus leading to a suppression of RNA by bacteria [28]. Rifampin is part of the recommended drugs used for the treatment of active TB during pregnancy (first-line medication to treat TB during pregnancy), although the safety of this drug during pregnancy is not yet known [29]. However, studies have indicated that the most severe side effect of rifampin is hepatotoxicity, and it is advisable that the patient receiving it should frequently undertake baseline and regular liver function tests for early detection of liver damage [30]. Other commonly reported side effects include diarrhea, nausea, loss of appetite and vomiting [31].
Streptomycin is one of the antibiotic medications used for the treatment of bacterial infections, including TB [32]. For the treatment of active TB, streptomycin is frequently used in combination with other antituberculosis drugs such as pyrazinamide, rifampicin and isoniazid [33,34]. However, streptomycin is not usually used as first-line treatment, except in medically under-served populations where the cost of more expensive treatments is prohibitive. Streptomycin works by two mechanisms depending on the isomer (conformation): (1) the streptomycin isomer A functions as a protein synthesis inhibitor. This occurs by binding the isomer A to the small 16S rRNA of the 30S subunit of the bacterial ribosome irreversibly, thereby interfering with the binding of formyl-methionyl-tRNA to the 30S subunit. (2) Streptomycin isomer B is an inhibitor of peptidoglycan synthesis inhibitor [35]. The isomer B binds to the glycosidic linkages and breaks them through an SN2 mechanism, thereby leading to the integrity of the bacterial cell walls being compromised, eventually resulting in the death of microbial cells [35]. Even though this drug is administered intravenously, several side effects have been reported, including rash, vertigo, numbness of the face and fever [36]. In addition, a report has also indicated that the use of streptomycin during pregnancy may cause permanent hearing loss in the developing baby [37].

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Antituberculosis agents with their limitations in the treatment of tuberculosis.
| Anti-Tuberculosis Agents | Mechanism of Action | Reported Side Effects | References |
|---|---|---|---|
| Ethambutol | Not known. | Vomiting, blurred vision, rash, nausea, swelling of the face, breathlessness. | [14] |
| Isoniazid | It inhibits the synthesis of mycolic acids (components of the mycobacterial cell wall), thereby interfering with cell wall synthesis. | Liver inflammation, numbness in hand and feet, liver failure, and increased blood levels of liver enzymes. | [16,17] |
| Linezolid | Prevents the initiation of bacterial protein synthesis. | Headache, nausea, difficulty breathing, swelling in face or throat. | [20,21] |
| Pyrazinamide | Intervenes with the nuclei acid metabolism of bacterial cells due to its structure similar to that of nicotinamide. | Liver injury, gastrointestinal upset, skin rashes, arthralgias, anorexia, nausea and vomiting. | [23,25] |
| Rifampin | Inhibit bacterial DNA-dependent RNA polymerase. | Hepatotoxicity. | [28,31] |
| Streptomycin | Blocks the ability of the 30S ribosomal subunits to make proteins. | Rash, vertigo, numbness of the face, fever, and rash. | [35,36] |
1.3. Medicinal Plants with Antituberculosis Properties
Due to the several reported side effects associated with the use of antituberculosis agents, many TB patients have now resorted to using several medicinal plants to treat TB [38,39,40]. These medicinal plants have been reported to contain numerous bioactive compounds with antimycobacterial activity [41]. Recently, there has been a search for medicinal plants with ethno-pharmacological abilities for the treatment of TB and several ethnobotanical studies have also documented these medicinal plants. For example, Gupta et al. [42] tested four plant (Allium sativum, Aloe vera, Acalypha indica and Allium cepa) extracts against the H37Rv strain of M. tuberculosis with a zone of inhibition between 2.5 and 17.3 mm at the tested concentrations (0.02–0.04 mg/mL). Mohamed et al. [43] also reported that the n-hexane partition of Costus speciosus, Cymbopogon citratus and Tabernaemontana coronaria exhibited anti-TB activity against M. tuberculosis H37Rv with minimum inhibitory concentrations (MICs) of 100–200 μg/mL and a minimum bactericidal concentration (MBC) of 200 μg/mL. In the study, the authors proposed that the antituberculosis activity of these extracts was due to their destructive effects on the integrity of the mycobacterial cellular structure. Another study conducted by Kahaliw et al. [44] reported that the chloroform extracts of Pterolobium stellatum exhibited anti-TB activity against M. tuberculosis strain H37RV with MIC values of 0.039 mg/mL. A review conducted by Xu et al. [45] also reported and compiled several medicinal plants as a source of anti-TB drugs. Kaur and Kaur [46] reported the antituberculosis activity of methanolic extract of Aegle marmelos, Glycyrrhiza glabra, Lawsonia inermis, Piper nigrum and Syzygium aromaticum microplate alamar blue assay. In the study, the extracts exhibited antituberculosis activity against M. tuberculosis strain H37RV at a range of 0.8 to 100 μg/mL. Interestingly, despite the widespread usage of medicinal plants for the management of TB, there are still many plants that are yet to be scientifically documented. It is in this context that this review focused on medicinal plants used as a combating strategy against TB in the Mpumalanga Province of South Africa with a view to prevent the loss of these important plants for future generations in the Mpumalanga Province.
2. Material and Methods
A detailed literature review was carried out (between August 2021 to January 2023). Information on plants traditionally used to manage TB in the Mpumalanga Province was obtained from numerous databases, namely PubMed, Medline, Scopus, Science Direct, Web of Science and Google Scholar. Additional information was also obtained from ethnobotanical books, dissertations and theses using various university libraries. Some of the keywords and terms used when searching for relevant articles or research papers were “Medicinal plants”, “tuberculosis”, “Mpumalanga”, and “ethnopharmacology”.
3. Results and Discussion
3.1. Medicinal Plants with Antituberculosis Potential Used in the Mpumalanga Province
Twenty-four plant species belonging to different botanical families have been reported by the people of Mpumalanga for the treatment of antituberculosis (Table 2). Some of these plant species have been scientifically validated (Table 3), and only nine are yet to be scientifically investigated for their antituberculosis activity. A broad description of some of these plants with isolated antituberculosis compounds (Figure 3) is given below.
3.2. Agapanthus inapertus
Agapanthus inapertus (Figure 4) is a plant belonging to the family Agapanthaceae. The plant grows in grassland and in between rocks in mountainous terrain, forming large clumps. The leaves of the plant are mainly erect while the flower stalk is about 0.8 m high [47]. A. inapertus is dispersed in the Mpumalanga Province of South Africa [47]. The plant is also found in the Limpopo province and Mozambique [47]. Traditionally, the tuber part of the plant is cooked, and the extract is then taken by the people of Mpumalanga Province for the treatment of tuberculosis [48]. The literature survey showed no reported antituberculosis activity of A. inapertus and its phytoconstituents.
3.3. Combretum hereroense
Combretum hereroense is a semi-deciduous shrub that grows to about 5–12 m in height [49]. The plant belongs to the family Combretaceae. The leaves of the plant are very simply shaped and obovate. The plant is found in the Mpumalanga, Gauteng, Limpopo and KwaZulu-Natal provinces [49]. In traditional medicine, the seed of the plant is burnt in a hut and the smoke is inhaled for the treatment of TB [50]. Magwenzi et al. [51] reported that C. hererosene exhibited no antimycobacterial effects against Mycobacterium aurum and Mycobacterium smegmatis at the tested concentrations but showed an efflux pumping inhibitory activity in Mycobacterium smegmatis. Another study reported by Masoko and Nxumalo [52] indicated that the acetone extracts of C. hereroense inhibited the growth of M. smegmatis with MIC value of 0.47 mg/mL. Despite the widely reported antituberculosis activity of C. hereroense, there has been no scientific information on its isolated antimycobacterial compounds.
3.4. Helichrysum odoratissimum
Helichrysum odoratissimum is an aromatic that belongs to the family of Asteraceae. H. odoratissimum is a perennial plant with tiny grey leaves [53]. The plant’s leaves can vary between being linear, oblong, lingulate, and lanceolate. It is found in Mpumalanga, Limpopo, and KwaZulu-Natal provinces [53]. It is also found in the mountains and coastal areas of the Eastern Cape province, South Africa [53]. The leaves or whole plant parts are used for the treatment of TB in the Mpumalanga Province [54]. The antituberculosis activity of H. odoratissimum has been reported in the literature. Several reports have indicated that the extract of H. odoratissium has antituberculosis activities. For example, a study revealed that the whole-plant extract demonstrated inhibition against M. tuberculosis at MICs ranging from 300 to 500 μg/mL [54]. Another study conducted by Seaman et al. [55] also indicated that the acetone extracts of H. odoratissimum inhibited M. smegmatis and M. aurum with MIC values range from 0.3 mg/mL to 2.0 mg/mL. No reported active antimycobacterial tuberculosis compound has been isolated from this plant.
3.5. Lippia javanica
Lippia javanica is a medicinal plant with dense creamy white flower heads and aromatic leaves. It is a woody shrub 1 to 2 m in height belonging to the family of Verbenaceae [56]. It is one of the most aromatic indigenous shrubs in South Africa [56]. The plant is prevalent throughout large parts of South Africa. The leaf of the plant is placed in water and the steam is inhaled to treat TB [57]. A study conducted by Masoko and Nxumalo revealed the antituberculosis activity of L. javanica against mycobacterial strains. In the study, the authors reported that L. javanica acetone extract displayed inhibition against M. smegmatis with an MIC value of 0.47 mg/mL [52]. Another study reported by Mujovo also showed that the acetone extract of L. javanica exhibited inhibition against M. tuberculosis (H37Rv) at a concentration of 0.5 mg/mL [58]. In the same study, 6-Methoxyluteolin 4′-methyl ether (1), a compound isolated from L. javanica, demonstrated significant inhibition against M. tuberculosis with an MIC value of 200 μg/mL [58].
3.6. Protorhus longifolia
Protorhus longifolia (Anacardiaceae family) is an excellent evergreen garden tree that is easily grown from seed. It is up to 15 m in height and single-stemmed with a dark rounded crown [59]. The leaves of the plants are simple, and are dark green with a paler underside. The plant is broadly distributed in the Eastern Cape, KwaZulu-Natal, Limpopo and Mpumalanga Provinces [59]. A decoction of the bark is taken orally to treat TB [60]. Some researchers have reported the antimycobacterial TB of P. longifolia [61]. A study conducted by Kabongo-Kayoka, reported that P. longifolia extract exhibited inhibition against M. aurum and M. fortuitum with an MIC value of 0.11 mg/mL [61]. The author also revealed that the plant extract also caused inhibition against M. smegmatis with an MIC value of 0.07 mg/mL [61]. Interestingly, another study reported by Mdikizela and McGaw also reported that P. longifolia leaf acetone extract reported good activity against M. smegmatis and M. bovis with MIC values of 0.008 mg/mL [62]. There have been no reports of antimycobacterial compounds isolated from this plant.
3.7. Phymaspermum acerosum
Phymaspermum acerosum is an erect straggly shrub that belongs to the Asteraceae family. The plant reaches a height and width of 1.5–2 m. The plant leaves are up to 10 to 45 mm long with a bright yellow flower [63]. P. acerosum is found in the Mpumalanga, Eastern Cape, Gauteng, Northern Province and Free State provinces of South Africa, as well as Lesotho [63]. In Mpumalanga Province, the infusion of the root is taken orally for TB management [60]. A report has indicated that P. acerosum roots and leaf (ethanol and water) extracts exhibited inhibition against the mycobacterium strain with an MIC value of 0.02 mg/mL [62]. There have been no reports of antimycobacterial compounds isolated from P. acerosum.
3.8. Ranunculus multifidus
Ranunculus multifidus is an evergreen herb that grows well in damp grassland. The plant is a flowering plant in the family Ranunculaceae. R. multifidus has bright green leaves that grow from a basal rosette and are covered with hairs, and is therefore described as an excellent candidate for an undercover spot [64]. The plant is naturally found across the Eastern Cape, KwaZulu-Natal, Limpopo, Mpumalanga, Northern Cape, Northwest and Western Cape provinces [65]. The infusion of the root is used for TB management [60]. Nevertheless, there is no scientific evidence of its antituberculosis properties yet, and there have been no reported antituberculosis compounds isolated from this plant.
3.9. Tetradenia riparia
Tetradenia riparia (Lamiaceace family) is a tall, aromatic plant that has a height of up to 3 m. The plant has glandular hairs that cover the surfaces of the leaves, thereby making them slightly sticky to the touch [66]. T. riparia leaves are light green, and they are softly heart-shaped with the margin intermittently and openly toothed. The natural distribution of the plant ranges from Mpumalanga, KwaZulu-Natal, and Northern Province in South Africa [66]. The plant is used traditionally as an infusion to treat respiratory diseases, including TB [67]. The anti-mycobacterium tuberculosis activity of essential oil from T. riparia was reported by Baldin et al. [68]. In that study, the authors discovered that the essential oil of T. riparia displayed inhibition against M. tuberculosis H37Rv with an MIC value of 62.5 µg/mL. Another study conducted by van Puyvelde et al. [69] also reported significant inhibition towards M. simiae and M. tuberculosis at the concentration of 1000 μg/mL and 500 μg/mL respectively. The compound, 6,7-dehydroroyleanone (6) isolated from T. riparia was reported to show activity against M. tuberculosis H37Rv with an MIC value of 62.5 µg/mL [68]. Another compound, 8(14), 15-sandaracopimaradiene-7α, 18-diol (7), also isolated from the T. riparia, was shown to exhibit antimycobacterial activity against M. tuberculosis at concentrations ranging from 25 μg/mL to 100 μg/mL [69].
3.10. Withania somnifera
Withania somnifera is a tiny flowering shrub belonging to the family Solanaceae. The whole plant is covered with short and branched hair and reaches 2 m high and 1 m across [70]. The plant leaves are simple, alternate, ovate and oblong with 30–80 mm long margins. W. somnifera is widespread in several provinces of South Africa, including Mpumalanga [70]. In Mpumalanga, the infusion of the plant is used against TB [71]. The literature search revealed some notable works on the antimycobacterial tuberculosis activity of W. somnifera. Adaikkappan et al. [72] discovered that W. somnifera aqueous extract showed a significant effect against M. tuberculosis at concentrations ranging from 0.01 to 1.0 mg/mL. There have been no reports on the antimycobacterial activity of active isolated compounds from W. somnifera.
3.11. Ziziphus mucronata
Ziziphus mucronate is a small to medium-sized plant 3–10 m in height. The plant belongs to the family of Rhamnaceae. The leaves of the plant are simple, alternate and broadly ovate in size [73]. Z. mucronata is mostly dispersed throughout the summer rainfall areas of sub-Saharan Africa, spreading from South Africa [73]. The plant is predominant in Mpumalanga, Eastern Cape, Free State, Gauteng and KwaZulu-Natal provinces [73]. Traditionally, the infusion prepared from the leaves is used to treat TB [71]. The acetone extract of Z. mucronata exhibited inhibition against M. tuberculosis with an MIC value of 0.156 mg/mL [74,75]. The authors also indicated that the extract displayed inhibition against M. fortuitum and M. aurum with an MIC value of 2.5 mg/mL [75]. Another study conducted by Iloga [76] revealed that dichloromethane extract of Z. mucronata demonstrated inhibition against M. terrae at MIC values of <0.156 mg/mL. A report by Sigidi et al. [77] revealed that Z. mucronata aqueous extract displayed an MIC value of >500 µg/mL against the pathogenic M. tuberculosis H37V strain. The literature search conducted showed no reported antimycobacterial compounds isolated from this plant.
Table 2.
Medicinal plants used traditionally to treat tuberculosis in the Mpumalanga Province of South Africa.
Table 2.
Medicinal plants used traditionally to treat tuberculosis in the Mpumalanga Province of South Africa.
| S/N | Scientific Name | Local Name | Family | Plant Part Used | Mode of Preparation/Administration | Reference |
|---|---|---|---|---|---|---|
| 1 | Agapanthus inapertus P.Beauv. subsp. Intermedius | isicakathi | Agapanthaceae | Tuber | The tuber part of the plant is cooked for 10 min, and the extract (one cup) is taken orally 3 times a day. | [48] |
| 2 | Combretum hereroense Schinz | umhlalavane | Combretaceae | Seeds | The seed of the plant is burnt in a hut and the smoke is inhaled 2 times a day. | [50] |
| 3 | Dicoma anomala Sond. | inyongana | Asteraceae | Leaves | The leaves of the plant are chewed. | [78] |
| 4 | Eucomis autumnalis (Mill.) Chitt | esimathunzi | Hyacinthaceae | Bulb | The infusion prepared from the bulbs is drunk for tuberculosis management. | [78] |
| 5 | Hypoxis hemerocallidea Fisch., C.A.Mey. & Avé-Lall. | lezithunzela | Hypoxidaceae | Tuber | The tuber of the plant is cooked for 5–20 min, and the extract (one cup) taken 3 times a day. | [48] |
| 6 | Helichrysum odoratissimum (L.) Sweet. | imphepho | Asteraceae | Leaves | Unspecified. | [79] |
| 7 | Heteromorpha arborescens (Spreng.) Cham. & Schltdl. | umbangeza | Apiaceae | Root | An infusion obtained from the root is taken orally. | [62] |
| 8 | Lippia javanica (Burm. f.) | umsutane | Verbenaceae | Leaves | The leaves of the plant are placed in water and the steam is inhaled 3 times a day. | [48,57] |
| 9 | Leonotis leonurus (L.) R.Br. | Lamiaceae | Leaves andstems | Unspecified. | [78] | |
| 10 | Merwilla plumbea (Lindl.) Speta | inguduza | Hyacinthaceae | Bulb | The bulb of the plant is cooked for approximately 8 min and the extract (on cup) is taken 3 times a day. | [48] |
| 11 | Mentha longifolia | ufuthana | Lamiaceae | Leaves | Infusion made from the leaves is taken orally 3 times a day for 2 months. | [71] |
| 12 | Pelargonium sidoides DC | iyeza | Geraniaceae | Tuber | Unspecified. | [78] |
| 13 | Pellaea calomelanos (Sw.) Link | inkomankomo | Pteridaceae | The infusion of the roots is prepared, and one cup of the extract is taken orally. | [48] | |
| 14 | Protorhus longifolia (Bernh.) Engl | isifuce | Anacardiaceae | Bark | An infusion of the bark is taken orally. | [60] |
| 15 | Phymaspermum acerosum (DC.) Källersjö | umhlonishwa | Asteraceae | Root | Infusion of the root is taken orally. | [60] |
| 16 | Ranunculus multifidus Forssk. | Unspecified | Ranunculaceaea | Root | Infusion of the root is taken orally. | [60] |
| 17 | Schotia latifolia Jacq. | umXamo | Fabaceae | Bark | The decoction of the bark is taken orally. | [60] |
| 18 | Strychnos henningsii Gilg | Umanono | Loganiaceae | Bark | The bark of the plant is chewed. | [60] |
| 19 | Silene undulata Aiton | ubulawu | Caryophyllaceae | Leaves | The infusion made from the leaves is taken orally. | [71] |
| 20 | Talinum caffrum (Thunb.) Eckl. & Zeyh. | impunyu | Talinaceae | Root | The decoction made from the root is taken orally | [60] |
| 21 | Tetradenia riparia (Hochst.) Codd | Ibozane | Lamiaceae | Leaves | The plant infusion is used to treat respiratory diseases, including tuberculosis | [79] |
| 22 | Withania somnifera (L.) Dunal | ubuvuma | Solanaceae | Leaves | Infusion from the herbs is taken orally | [71] |
| 23 | Xysmalobium undulatum (L.) Aiton f. var. undulatum | nwachaba | Apocynaceae | Whole plant | Unspecified | [78] |
| 24 | Ziziphus mucronata (Willd subsp) | Rhamnaceae | Leaves | The infusion prepared from the leaves is taken orally | [71] |
Table 3.
Reported antituberculosis activity of medicinal plants used in the Mpumalanga Province.
| S/N | Scientific Name | Plant Part Used | Extract | Antimycobacterial Isolated Compounds | Antituberculosis Mechanism of Action | References |
|---|---|---|---|---|---|---|
| 1 | C. hereroense | * | * | * | Exhibited no activity against Mycobacterium aurum and Mycobacterium smegmatis. Exhibited efflux pumping inhibitory activity in Mycobacterium smegmatis | [51] |
| 2 | D. anomala. | Leaves | Acetone, Ethanol | * | Inhibited Mycobacterial tuberculosis at MIC values of 0.195 mg/mL. | [78] |
| 3 | E. autumnalis | Bulb | Aqueous | * | Displayed inhibition against Mycobacterial tuberculosis at MIC values of 3.125 mg/mL. | [78] |
| 4 | H. odoratissimum | Leaves | Acetone | * | Inhibited Mycobacterial tuberculosis at MIC values of 0.5 mg/mL. | [80] |
| 5 | H. arborescens | Leaves | Aqueous, acetone, and ethanol leaf extracts | * | Displayed inhibition against M. aurum, M. bovis, M. bovis BCG, M. gordonae, M. fortuitum, M. smegmatis, M. tuberculosis and M. tuberculosis H37RV with MIC values ranging between 0.08 mg/mL to 5.0 mg/mL. | [62,81] |
| 6 | L. javanica | Leaves | Acetone | 6-Methoxyluteolin 4′-methyl ether (1) | The acetone extract displayed inhibition against M. smegmatis with an MIC value of 0.47 mg/mL. The isolated compound “6-Methoxyluteolin 4′-methyl ether” exhibited an MIC value of 200 µg/mL against M. tuberculosis. | [52,58] |
| 7 | L. leonurus | Leaves | Aqueous | * | No activity against M. smegmatis | [79] |
| 8 | P. sidoides | Root | Butanol | Epigallocatechin (2), scopoletin (3), catechin (4) and umckalin (5) | The butanol extract displayed inhibition against M. tuberculosis H37Rv. The isolated compounds (epigallocatechinand scopoletin) showed good inhibitory activity against M. smegmatis, thereby exhibiting a MIC value of 7.8 mg/mL. Another isolated compound (catechin and umckalin) inhibited M. smegmatis with a MIC value of 31.25 and 62.5 mg/mL respectively. | [82,83] |
| 9 | P. longifolia | Leaves | Acetone | * | Inhibited M. aurum and M. fortuitum with an MIC value of 0.11 mg/mL while for the M. smegmatis with an MIC value of 0.07 mg/mL. | [61] |
| 10 | P. acerosum | Root | Water and Ethanol | * | Inhibited Mycobacterium strain with an MIC value of 0.02 mg/mL | [62] |
| 11 | T. caffrum | Rhizome | Acetone | * | Displayed no antituberculosis activity against Mycobacterium strains | [62] |
| 12 | T. riparia | leaves | Essential oil | 6,7-dehydroroyleanone (6), 8(14), 15-sandaracopimaradiene-7α, 18-diol (7) | The essential oil displayed inhibition against M. tuberculosis H37Rv MIC value of 62.5 µg/mL. The isolated compound (6,7-dehydroroyleanone) inhibited M. tuberculosis H37Rv with an MIC value of 62.5 µg/mL while, 8(14), 15-sandaracopimaradiene-7α, 18-diol inhibited M. tuberculosis between the concentration range of 25 μg/mL to 100 μg/mL | [68] |
| 13 | W. somnifera | leaves | Aqueous | * | Exhibited inhibition against M. tuberculosis H37Rv between 0.01–1.0 mg/mL | [72] |
| 14 | X. undulatum | Leaves | Methanol | * | Displayed no inhibition against M. tuberculosis | [78] |
| 15 | Z. mucronata | Bark | Ethanol | * | No inhibition against M. smegmatis and M. tuberculosis | [84] |
*: No reported antimycobacterial isolated compound.
Figure 4.
Medicinal plants used traditionally to treat tuberculosis in Mpumalanga Province. Pictures obtained from SANBI [85].
Figure 4.
Medicinal plants used traditionally to treat tuberculosis in Mpumalanga Province. Pictures obtained from SANBI [85].




4. Conclusions and Recommendations
In the Mpumalanga Province, the number of people using herbs for the treatment of TB is steadily increasing. This is ascribed to their cultural beliefs, low cost, availability, and efficacy of these medicinal plants in combating tuberculosis. However, despite their usage, many of these plants have not been scientifically explored. Thus, there is a need for researchers or pharmaceutical industries to explore these species. It is also important that efforts should be made to isolate more antimycobacterial compounds that can be developed into new anti-tuberculosis drugs with better efficacy and safety profiles.
Author Contributions
Conceptualization: I.J.S. and A.A.H.; Methodology: I.J.S. and A.A.H.; Resources: A.A.H. Investigation: I.J.S.; Writing of the original draft: I.J.S.; Editing: I.J.S. and A.A.H.; Supervision: A.A.H. All authors have read and agreed to the published version of the manuscript.
Funding
This review work received no research/external funding.
Institutional Review Board Statement
No ethical approval was required for this review article.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors thank the Cape Peninsula University of Technology, for publication support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization (WHO). Global Report on Tuberculosis; WHO: Geneva, Switzerland, 2021; Available online: https://www.who.int/publications/i/item/9789240037021 (accessed on 24 February 2023).
- Pereira, M.; Tripathy, S.; Indamdar, V.; Ramesh, K.; Bhavsar, M.; Date, A.; Iyyer, R.; Acchammachary, A.; Mehendale, S.; Risbu, A. Drug resistance pattern of Mycobacterium tuberculosis in seropositive and seronegative HIV-TB patients in Pune, India. Indian J. Med. Res. 2005, 121, 235–239. [Google Scholar]
- Centre for Diseases Control and Prevention (CDC). Transmission and Pathogenesis of Tuberculosis. Available online: https://www.cdc.gov/tb/education/corecurr/pdf/chapter2.pdf (accessed on 24 December 2022).
- Nall, R. Tuberculosis. Healthline. 2021. Available online: https://www.healthline.com/health/tuberculosis (accessed on 24 January 2023).
- Sheer, W.T.; Coyle, T.A. Gastrointestinal tuberculosis. Curr. Gastroenterol. Rep. 2003, 5, 273–278. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). TB, A Global Emergency; WHO: Geneva, Switzerland, 1994; Available online: https://apps.who.int/iris/bitstream/handle/10665/58749/WHO_TB_94.177.pdf?sequence=1&isAllowed=y (accessed on 24 February 2023).
- World Health Organization (WHO). Tuberculosis; WHO: Geneva, Switzerland, 2022; Available online: https://www.who.int/news-room/fact-sheets/detail/tuberculosis (accessed on 28 February 2023).
- National Institute for Communicable Diseases (NCID). The First National TB Survey. 2018. Available online: https://www.nicd.ac.za/wp-content/uploads/2021/02/TB-Prevalence-survey-report_A4_SA_TPS-Short_Feb-2021.pdf (accessed on 17 March 2023).
- Mpumalanga Provincial Government (MPG). Remarks by Premier, R.M. Mtshweni-Tsipane on the Occasion of the Commemoration of World TB Day. 2021. Available online: http://www.mpumalanga.gov.za/media/speeches/otp/24032021.htm (accessed on 12 March 2023).
- Mashamba, M.A.; Tanser, F.; Afagbedzi, S.; Beke, A. Multi-drug-resistant tuberculosis clusters in Mpumalanga province, South Africa, 2013–2016: A spatial analysis. Trop. Med. Int. Health 2022, 27, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Selala, M.E.; Kgole, J.C.; Lekhuleni, M.E.; Jali, M.N. Factors influencing increase in tuberculosis patients in Mpumalanga Province. Afr. J. Phys. Act. Health Sci. 2013, 19, 518–526. [Google Scholar]
- Yew, W.W.; Lange, C.; Leung, C.C. Treatment of tuberculosis: Update 2010. Eur. J. Respir. 2011, 37, 441–462. [Google Scholar] [CrossRef]
- Dew, R.H. Ethambutol: An Overview. Available online: https://www.uptodate.com/contents/ethambutol-an-overview (accessed on 28 August 2022).
- Jnawali, H.N.; Ryoo, S. First– and Second–Line Drugs and Drug Resistance. In Tuberculosis—Current Issues in Diagnosis and Management. 2013. Available online: https://www.intechopen.com/chapters/43723 (accessed on 28 September 2022).
- National Institutes of Health (NIH). LiverTox: Clinical and Research Information on Drug Induced Liver Injury: Isoniazid. 2018. Available online: https://www.ncbi.nlm.nih.gov/books/NBK548754/ (accessed on 28 January 2023).
- Berning, S.E.; Peloquin, C.A. Antimycobacterial agents: Isoniazid. In Antimicrobial Therapy and Vaccines; Yu, V., Merigan, T., Barriere, S., Eds.; Williams and Wilkins: Baltimore, MD, USA, 1998. [Google Scholar]
- Mayo Clinic. Isoniazid (Oral Route, Intramuscular Route). Available online: https://www.mayoclinic.org/drugs-supplements/isoniazid-oral-route-intramuscular-route/side-effects/drg-20064419 (accessed on 13 March 2023).
- MedlinePlus. Linezolid. Available online: https://medlineplus.gov/druginfo/meds/a602004.html#:~:text=Linzolid%20is%20used%20to%20treat,flu%2C%20and%20other%20viral%20infections (accessed on 10 March 2023).
- World Health Organization (WHO). Consolidated Guidelines on Drug-Resistant Tuberculosis Treatment; WHO: Geneva, Switzerland, 2019; Available online: https://www.who.int/ (accessed on 28 February 2023).
- Ament, P.W.; Jamshed, N.; Horne, J.P. Linezolid: Its role in the treatment of gram-positive, drug-resistant bacterial infections. Am. Fam. Physician. 2002, 65, 663–671. [Google Scholar] [PubMed]
- Roger, C.; Roberts, J.A.; Muller, L. Clinical pharmacokinetics and pharmacodynamics of Oxazolidinones. Clin. Pharmacokinet. 2018, 57, 559–575. [Google Scholar] [CrossRef]
- Heifets, L. Antimycobacterial agents: Pyrazinamide. In Antimicrobial Therapy and Vaccines; Yu, V.L., Merigan, T.C., Barriere, S.L., Eds.; Williams and Wilkins: Baltimore, MD, USA, 1999. [Google Scholar]
- Verma, S.; Kaplowitz, N. Hepatotoxicity of antitubercular drugs in drug-Induced liver disease. In Drug-Induced Liver Disease, 3rd ed.; Kaplowitz, N., DeLeve, L.D., Eds.; Elsevier: London, UK, 2013; pp. 483–504. [Google Scholar]
- Chiang, S.S.; Starke, J.R. Mycobacterium tuberculosis. In Principles and Practice of Pediatric Infectious Diseases, 5th ed.; Long, S.S., Ficher, M., Prober, C.G., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 790–806. [Google Scholar]
- Knobel, B.; Buyanowsky, G.; Dan, M.; Zaidel, L. Pyrazinamide-Induced granulomatous Hepatitis. J. Clin. Gastroenterol. 1997, 24, 264–266. [Google Scholar] [CrossRef]
- National Institutes of Health (NIH). LiverTox: Clinical and Research Information on Drug Induced Liver Injury: Pyrazinamide. 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK547856/ (accessed on 12 September 2022).
- World Health Organization (WHO). Treatment of Tuberculosis: Guidelines, 4th ed.; WHO: Geneva, Switzerland, 2010; Available online: https://apps.who.int/iris/handle/10665/44165 (accessed on 28 February 2023).
- Calvori, C.; Frontali, L.; Leoni, L.; Tecce, G. Effect of rifamycin on protein synthesis. Nature 1965, 207, 417–418. [Google Scholar] [CrossRef]
- Bothamley, G. Drug Treatment for tuberculosis during pregnancy. Drug Saf. 2001, 24, 553–565. [Google Scholar] [CrossRef]
- Chang, T.-E.; Huang, Y.-S.; Su, W.-J.; Perng, C.-L.; Huang, Y.-H.; Hou, M.-C. The role of regular liver function monitoring in antituberculosis drug-induced liver injury. J. Chin. Med. Assoc. 2019, 82, 535–540. [Google Scholar] [CrossRef]
- MedlinePlus. Rifampin. Available online: https://medlineplus.gov/druginfo/meds/a682403.html (accessed on 14 February 2023).
- Ruiz, P.; Rodríguez-Cano, F.; Zerolo, F.J.; Casal, M. Streptomycin as second-line chemotherapy for tuberculosis. Rev. Esp. Quimioter. 2003, 16, 188–194. [Google Scholar] [PubMed]
- Lienhardt, C.; Vernon, A.; Raviglione, M.C. New drugs and new regimens for the treatment of tuberculosis: Review of the drug development pipeline and implications for national programmes. Curr. Opin. Pulm. Med. 2010, 16, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Honeyborne, I.; Lipman, M.; Zumla, A.; McHugh, T.D. The changing treatment landscape for MDR/XDR-TB—Can current clinical trials revolutionise and inform a brave new world? Int. J. Infect. Dis. 2019, 80, S23–S28. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.; Cukras, A.R.; Rogers, E.J.; Southworth, D.R.; Green, R. Mutational analysis of S12 protein and Implications for the accuracy of decoding by the ribosome. J. Mol. Biol. 2007, 374, 1065–1076. [Google Scholar] [CrossRef]
- RxList. Streptomycin. Available online: https://www.rxlist.com/streptomycin-drug.htm (accessed on 14 February 2023).
- Donald, P.R.; Sellars, S.L. Streptomycin ototoxicity in the unborn child. S. Afr. Med. J. 1981, 60, 316–318. [Google Scholar]
- Oryema, C.; Rutaro, K.; Oyet, S.W.; Malinga, G.M. Ethnobotanical plants used in the management of symptoms of tuberculosis in rural Uganda. Trop. Med. Health 2021, 49, 92. [Google Scholar] [CrossRef]
- Getachew, S.; Medhin, G.; Asres, A.; Abebe, G.; Ameni, G. Traditional medicinal plants used in the treatment of tuberculosis in Ethiopia: A systematic review. Heliyon 2022, 8, e09478. [Google Scholar] [CrossRef]
- Tabuti, J.R.S.; Kukunda, C.B.; Waako, P.J. Medicinal plants used by traditional medicine practitioners in the treatment of tuberculosis and related ailments in Uganda. J. Ethnopharmacol. 2010, 127, 130–136. [Google Scholar] [CrossRef]
- Swain, S.S.; Hussain, T.; Pati, S. Drug-lead anti-tuberculosis phytochemicals: A Systematic Review. Curr. Top. Med. Chem. 2021, 21, 1832–1868. [Google Scholar] [CrossRef]
- Gupta, R.; Thakur, B.; Singh, P.; Singh, H.B.; Sharma, V.B.; Katoch, V.M.; Chauhan, S.V.S. Anti-tuberculosis activity of selected medicinal plants against multi-drug resistant Mycobacterium tuberculosis isolates. Indian J. Med. Res. 2010, 131, 809–813. [Google Scholar] [PubMed]
- Mohamad, S.; Ismail, N.N.; Parumasivam, T.; Ibrahim, P.; Osman, H.; Wahab, A.H. Antituberculosis activity, phytochemical identification of Costus speciosus (J. Koenig) Sm., Cymbopogon citratus (DC. Ex Nees) Stapf., and Tabernaemontana coronaria (L.) Willd. and their effects on the growth kinetics and cellular integrity of Mycobacterium tuberculosis H37Rv. BMC Complement. Altern. Med. 2018, 18, 5. [Google Scholar] [CrossRef]
- Kahaliw, W.; Aseffa, A.; Abebe, M.; Teferi, M.; Engidawork, E. Evaluation of the antimycobacterial activity of crude extracts and solvent fractions of selected Ethiopian medicinal plants. BMC Complement. Altern. Med. 2017, 17, 143. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Liang, B.; Kong, C.; Sun, Z. Traditional medicinal plants as a source of antituberculosis drugs: A system review. Biomed. Res. Int. 2021, 2021, 9910365. [Google Scholar] [CrossRef] [PubMed]
- Kaur, R.; Kaur, H. Antitubercular activity and phytochemical screening of selected medicinal plants. Orient. J. Chem. 2015, 31, 597–600. [Google Scholar] [CrossRef]
- SANBI (South African National Biodiversity Institute). Agapanthus inapertus . Available online: https://pza.sanbi.org/agapanthus-inapertus (accessed on 14 March 2023).
- Semenya, S.S.; Maroyi, A. Medicinal plants used for the treatment of tuberculosis by Bapedi traditional healers in three districts of the Limpopo Province, South Africa. Afr. J. Tradit. Complement. Altern. Med. 2013, 10, 316–323. [Google Scholar] [CrossRef]
- SANBI (South African National Biodiversity Institute). Combretum hereroense . Available online: http://pza.sanbi.org/combretum-hereroense (accessed on 14 March 2023).
- Breyer-Brandwijk, M.G.; Watt, J.M. The Medicinal and Poisonous Plants of Southern and Eastern Africa, 2nd ed.; Livingstone: London, UK, 1962. [Google Scholar]
- Magwenzi, R.; Nyakunu, C. The effect of selected Combretum Species from Zimbabwe on the growth and drug efflux systems of Mycobacterium aurum and Mycobacterium smegmatis. J. Microb. Biochem. Technol. 2011, S3, 1–7. [Google Scholar] [CrossRef]
- Masoko, P.; Nxumalo, K.M. Validation of antimycobacterial plants used by traditional healers in three districts of the Limpopo Province (South Africa). Evid. Based Complement. Altern. Med. 2013, 2013, 586247. [Google Scholar] [CrossRef]
- Akinfenwa, A.O.; Sagbo, I.J.; Makhaba, M.; Mabusela, W.T.; Hussein, A.A. Helichrysum genus and compound activities in the management of diabetes mellitus. Plants 2022, 11, 1386. [Google Scholar] [CrossRef]
- McGaw, L.J.; Lall, N.; Meyer, J.J.M.; Eloff, J.N. The potential of South African plants against Mycobacterium infections. J. Ethnopharmacol. 2008, 119, 482–500. [Google Scholar] [CrossRef]
- Seaman, T. The Antimicrobial and Antimycobacterial Activity of Plants Used for the Treatment of Respiratory Ailments in Southern Africa and the Isolation of Anacardic Acid from Ozoroa paniculosa. Master’s Thesis, University of the Witwatersrand, Johannesburg, South Africa, 2005. [Google Scholar]
- SANBI (South African National Biodiversity Institute). Lippia javanica . Available online: https://pza.sanbi.org/lippia-javanica (accessed on 14 March 2023).
- Green, E.; Samie, A.; Obi, C.L.; Besson, P.O.; Ndip, R.N. Inhibitory properties of selected South African medicinal plants against Mycobacterium tuberculosis. J. Ethnopharmacol. 2010, 130, 151–157. [Google Scholar] [CrossRef]
- Mujovo, S.F. Antimicrobial activity of compounds isolated from Lippia javanica (Burm.f.) Spreng and Hoslundia opposita against Mycobacterium tuberculosis and HIV-1 Reverse transcriptase. Ph.D. Thesis, University of Pretoria, Hatfield, South Africa, 2009. [Google Scholar]
- SANBI (South African National Biodiversity Institute). Protorhus longifolia . Available online: https://pza.sanbi.org/protorhus-longifolia (accessed on 14 March 2023).
- Madikizela, B.; Kambizi, L.; McGaw, L.J. An ethnobotanical survey of plants used traditionally to treat tuberculosis in the eastern region of O.R. Tambo district, South Africa. S. Afr. J. Bot. 2017, 109, 231–236. [Google Scholar] [CrossRef]
- Kabongo-Kayoka, P.N.; Eloff, J.N.; Obi, C.L.; McGaw, L.J. Antimycobacterial activity and low cytotoxicity of leaf extracts of some African Anacardiaceae tree species. Phytother. Res. 2016, 30, 2001–2011. [Google Scholar] [CrossRef]
- Madikizela, B.; McGaw, L.J. Scientific rationale for traditional use of plants to treat tuberculosis in the eastern region of the OR Tambo district, South Africa. J. Ethnopharmacol. 2018, 224, 250–260. [Google Scholar] [CrossRef] [PubMed]
- SANBI (South African National Biodiversity Institute). Phymaspermum acerosum . Available online: http://pza.sanbi.org/phymaspermum-acerosum (accessed on 17 March 2023).
- Wild Flower Nursery. Ranunculus multifidus . Available online: https://wildflowernursery.co.za/indigenous-plant-database/ranunculus-multifidus/ (accessed on 17 March 2023).
- SANBI (South African National Biodiversity Institute). Red List of South African Plants. Available online: http://redlist.sanbi.org/species.php?species=2013-4/ (accessed on 18 March 2023).
- SANBI (South African National Biodiversity Institute). Tetradenia riparia . Available online: http://pza.sanbi.org/tetradenia-riparia (accessed on 10 March 2023).
- Panda, S.K.; Gazim, Z.C.; Swain, S.S.; Bento, M.C.V.D.; Sena, J.D.S.; Mukazayire, M.J.; Puyvelde, L.V.; Luyten, W. Ethnomedicinal, phytochemical and pharmacological Investigations of Tetradenia riparia (Hochst.) Codd (Lamiaceae). Front. Pharmacol. 2022, 13, 896078. [Google Scholar] [CrossRef] [PubMed]
- Baldin, V.P.; Scodro, R.B.D.; Lopes-Ortiz, M.A.; de Almeida, A.L.; Gazim, Z.L.; Ferarrese, L.; dos Santos Faiões, V.; Torres-Santos, E.C.; Pires, C.T.A.; Caleffi-Ferracioli, K.R.; et al. Anti-mycobacterium tuberculosis activity of essential oil and 6, 7-dehydroroyleanone isolated from leaves of Tetradenia riparia (Hochst.) Codd (Lamiaceae). Phytomedicine 2018, 47, 34–39. [Google Scholar] [CrossRef]
- van Puyvelde, L.; Ntawukiliyayo, J.D.; Portaels, F.; Hakizamungu, E. In vitro inhibition of mycobacteria by Rwandese medicinal plants. Phytother. Res. 1994, 8, 65–69. [Google Scholar] [CrossRef]
- SANBI (South African National Biodiversity Institute). Withania somnifera . Available online: http://pza.sanbi.org/withania-somnifera (accessed on 17 March 2023).
- Lawal, I.O.; Grierson, D.S.; Afolayan, A.J. Phytotherapeutic Information on plants used for the treatment of tuberculosis in Eastern Cape Province, South Africa. Evid. Based Complement. Alternat. Med. 2014, 2014, 735423. [Google Scholar] [CrossRef]
- Adaikkappan, P.; Kannapiran, M.; Anthonisamy, A. Anti-mycobacterial activity of Withania somnifera and Pueraria tuberosa against Mycobacterium tuberculosis H37Rv. J. Acad. Indus. Res. 2012, 1, 53–156. [Google Scholar]
- SANBI (South African National Biodiversity Institute). Ziziphus mucronata . Available online: http://pza.sanbi.org/ziziphus-mucronata (accessed on 17 March 2023).
- Dzoyem, J.P.; Aro, A.O.; McGaw, L.J.; Eloff, J.N. Antimycobacterial activity against different pathogens and selectivity index of fourteen medicinal plants used in southern Africa to treat tuberculosis and respiratory ailments. S. Afr. J. Bot. 2016, 102, 70–74. [Google Scholar] [CrossRef]
- Mongalo, N.I.; Mashele, S.S.; Makhafola, T.J. Ziziphus mucronata Willd. (Rhamnaceae): It’s botany, toxicity, phytochemistry and pharmacological activities. Heliyon 2020, 6, e03708. [Google Scholar] [CrossRef] [PubMed]
- Ilonga, S.K. Anticancer, Antioxidant and Antimicrobial Screening of Extracts from Ziziphus mucronata, Heliotropium ciliatum and Gnidia polycephala from the Oshikoto Region of Namibia. Master’s Thesis, University of Namibia, Windhoek, Namibia, 2012. [Google Scholar]
- Sigidi, M.T.; Anokwuru, C.P.; Zininga, T.; Tshisikhawe, M.P.; Shonhai, A.; Ramaite, I.D.I.; Traore, A.N.; Potgieter, N. Comparative in vitro cytotoxic, anti-inflammatory and anti-microbiological activities of two indigenous Venda medicinal plants. Transl. Med. Commun. 2016, 1, 9. [Google Scholar] [CrossRef]
- Hlongwane, M. Bioactivity of Traditional Medicinal Plants used in the Treatment of Tuberculosis in the Free State, South Africa. Master’s Thesis, University of Free State, Bloemfontein, South Africa, 2016. [Google Scholar]
- Singh, A. Bioactive Compounds from South African Plants against Mycobacterium tuberculosis. Ph.D. Thesis, Durban University of Technology, Durban, South Africa, 2016. [Google Scholar]
- Lall, N.; Meyer, J.J.M. In vitro inhibition of drug-resistant and drug-sensitive strains of Myco-bacterium tuberculosis by ethnobotanically selected South African plants. J. Ethnopharmacol. 1999, 66, 347–354. [Google Scholar] [CrossRef]
- Maroyi, A. Heteromorpha arborescenes: A review of its botany, medicinal uses, and pharmacological properties. Asian J. Pharm. Clin. Res. 2018, 11, 75–82. [Google Scholar] [CrossRef]
- Mativandlela, S.P.N.; Lall, N.; Meyer, J.J.M. Antibacterial, antifungal and antitubercular activity of (the roots of) Pelargonium reniforme (CURT) and Pelargonium sidoides (DC) (Geraniaceae) root extracts. S. Afr. J. Bot. 2006, 72, 232–237. [Google Scholar] [CrossRef]
- Mativandlela, S.P.N.; Meyer, J.J.M.; Hussein, A.A.; Lall, N. Antitubercular activity of Compounds Isolated from Pelargonium sidoides. Pharm. Biol. 2007, 45, 645–650. [Google Scholar] [CrossRef]
- Mativandlela, S.P.N.; Meyer, J.J.M.; Hussein, A.A.; Houghton, P.J.; Hamilton, C.J.; Lall, N. Activity against Mycobacterium smegmatis and Mycobacterium tuberculosis by extract of South African medicinal plants. Phytother. Res. 2008, 22, 841–845. [Google Scholar] [CrossRef]
- SANBI (South African National Biodiversity Institute). Available online: https://pza.sanbi.org/ (accessed on 17 March 2023).
Figure 1.
Typical symptoms of TB.

Figure 2.
The chemical structure of antituberculosis drugs.

Figure 3.
Antimycobacterial tuberculosis compounds isolated from plants used against tuberculosis in Mpumalanga Province. The numbers 1 to 7 correspond to the compound reported in Table 2.
Figure 3.
Antimycobacterial tuberculosis compounds isolated from plants used against tuberculosis in Mpumalanga Province. The numbers 1 to 7 correspond to the compound reported in Table 2.


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Sagbo, I.J.; Hussein, A.A. Are Plants Used as a Combating Strategy against Tuberculosis in the Mpumalanga Province, South Africa? Appl. Sci. 2023, 13, 5008. https://doi.org/10.3390/app13085008
AMA Style
Sagbo IJ, Hussein AA. Are Plants Used as a Combating Strategy against Tuberculosis in the Mpumalanga Province, South Africa? Applied Sciences. 2023; 13(8):5008. https://doi.org/10.3390/app13085008
Chicago/Turabian StyleSagbo, Idowu Jonas, and Ahmed A. Hussein. 2023. "Are Plants Used as a Combating Strategy against Tuberculosis in the Mpumalanga Province, South Africa?" Applied Sciences 13, no. 8: 5008. https://doi.org/10.3390/app13085008
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.